What happens when you crack a tooth depends on how deep the crack goes. A surface crack may cause no symptoms. A crack into the inner layer causes pain when biting and temperature sensitivity. A crack reaching the pulp (the living nerve tissue inside the tooth) requires root canal treatment to save the tooth. A crack into the root usually means the tooth cannot be saved.
What happens when you crack a tooth depends entirely on the depth and direction of the crack. A superficial crack in the enamel (the hard outer shell of the tooth, the hardest substance in the human body) only may cause no symptoms and require no treatment. A crack extending into the dentin (the layer of tooth beneath the hard enamel, softer and more sensitive, containing microscopic channels that connect to the nerve) causes pain when biting and temperature sensitivity. If the crack reaches the pulp (the soft living tissue inside the tooth, containing nerves and blood vessels), the pulp becomes inflamed and eventually infected, requiring root canal treatment to save the tooth. A crack that extends into the root almost always means the tooth cannot be saved. Acting at the earliest sign of a crack gives you the best chance of a simple, successful outcome.
You bite down on something hard, a popcorn kernel, a piece of ice, a hard candy, and feel that unmistakable sharp sensation. Or perhaps a tooth cracked during normal chewing, which happens more often than people realize. Whatever caused it, the question is the same: what happens now, and what should you do?
The answer depends on a series of clinical factors that your dentist and endodontic specialist will evaluate. Cracks are a common problem, and where the crack stops determines almost everything about your treatment and prognosis.5 Here is how cracks progress and what each stage means for treatment.
The Progression of an Untreated Crack
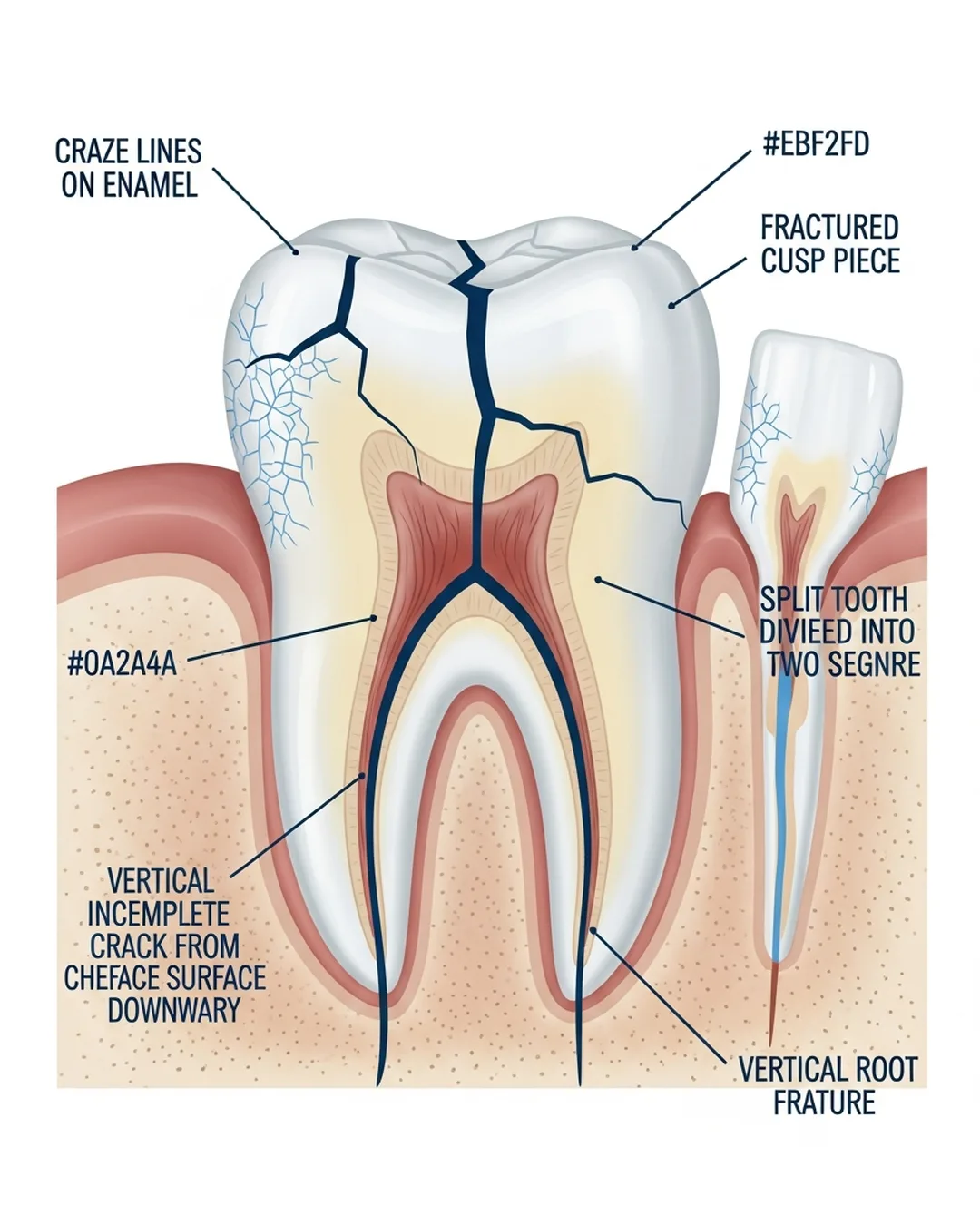
Surface crack, no symptoms
Stage 1. Enamel Only (Craze Line) Microscopic cracks in the outer enamel layer only. Extremely common in adults. Causes no pain, no sensitivity, and poses no structural threat.5 No treatment needed beyond monitoring. Cosmetic bonding is an option if visible aesthetically.

Pain with biting, temperature sensitivity
Stage 2. Into Dentin (Incomplete Fracture) The crack has extended through enamel into dentin but has not reached the pulp. Sharp, directional pain when biting, often with rebound pain on releasing the bite, is the hallmark. Brief cold sensitivity may appear. This is the ideal treatment window. A full-coverage crown placed now can protect the pulp from bacterial infiltration, stabilize the crack, and often eliminate symptoms without a root canal. Research shows that covering a cracked tooth with a full crown, rather than a direct filling that leaves the cusps unprotected, significantly lowers the risk of later pulp complications and tooth loss.1
Spontaneous pain, lingering sensitivity
Stage 3. Pulp Involvement (Irreversible Pulpitis) Bacteria or mechanical irritation from the crack has reached the pulp. The pulp is now irreversibly inflamed, too damaged to recover on its own. Spontaneous, throbbing pain may develop. Lingering cold sensitivity is present. Root canal treatment is now required before a crown can be placed. The tooth is still saveable at this stage, and root canal treatment remains a reliable way to keep a cracked tooth.2 The treatment is more involved than at Stage 2, and a full crown afterward gives the tooth its best long-term outlook.1

Infection, swelling, possible systemic signs
Stage 4, pulp necrosis (tissue death, when the living tissue inside a tooth dies due to infection or loss of blood supply) (death of the living tissue inside the tooth) and Abscess The pulp has died and bacteria have spread beyond the root tip, forming an abscess. Severe throbbing, swelling, possible fever. Root canal treatment is needed promptly. Healing takes longer because bone around the root has already been lost, but the tooth can still typically be saved with appropriate treatment.2
Tooth usually cannot be saved
Stage 5. Crack Extends to the Root (Vertical Root Fracture) The crack has propagated into the root itself. This is typically the endpoint of a crack that has been left untreated over a long period. A crack that runs from the chewing surface down into the root tends to carry a poor prognosis and often shows bone loss along the root.4 Vertical root fractures produce characteristic bone loss around the root that we can see on 3D CBCT (cone-beam CT, a low-dose 3D X-ray that lets us see the tooth and bone from every angle) imaging. In most cases, the tooth cannot be restored and requires extraction, followed by implant or bridge placement.
Can the Tooth Be Saved?
Tooth Can Usually Be Saved
- Crack confined to enamel and dentin (above the gumline)
- Pulp not yet involved, crown may be sufficient
- Pulp involved but intact, root canal + crown
- Active abscess present but crack doesn’t extend to root
- Treatment sought promptly after symptoms appear
Tooth Often Cannot Be Saved
- Vertical root fracture running along the root length
- Crack extends below the bone level
- Tooth is split completely into two separate pieces
- Insufficient remaining tooth structure for a crown
- Significant bone loss around the fractured root
What to Do Immediately After Cracking a Tooth
- Contact your dentist or endodontist promptly even if pain is mild, a crack needs professional assessment. The window between a saveable and an unsaveable tooth can close faster than expected
- Avoid chewing on the affected side continued bite forces can drive the crack deeper toward the root
- Avoid hard, crunchy, or sticky foods until the tooth has been evaluated and treated
- Take medications as recommended by your provider for any pain or discomfort
- Do not apply heat or cold to the outside of your face this can worsen swelling if infection is involved
- If a piece of tooth has broken off save it in milk or saliva and bring it to your appointment, in some cases it can inform the treatment plan
Referral note: Your general dentist is the right first call for a cracked tooth. They will assess the damage, take X-rays, and refer you to an endodontic specialist if pulp involvement is suspected or if the crack is difficult to evaluate without advanced imaging. Some insurance plans require a referral for specialist coverage.
Crack propagation is a well-documented progressive process in the dental literature. A 2024 systematic review and meta-analysis in the Journal of Dentistry found that cracked teeth restored with a full-coverage crown had a significantly lower risk of pulp complications and extraction than those given a direct filling that left the cusps unprotected, and the authors strongly recommended full-crown restoration for symptomatic cracked teeth and for cracked teeth that have had root canal treatment.1 Outcome studies of cracked teeth that received root canal treatment report favorable survival, with reported survival around 90 percent at two years in one cohort and roughly 84 percent at five years in a pooled analysis, underscoring that a cracked tooth caught and treated before the crack reaches the root usually has a good prognosis.23 Once a crack extends from the chewing surface into the pulp and down toward the root, the prognosis falls and bone loss along the root becomes more likely, which is why prompt assessment of pulp status at the time of diagnosis matters so much.4
Works Cited
- Zhang S, Xu Y, Ma Y, Zhao W, Jin X, Fu B. The treatment outcomes of cracked teeth: a systematic review and meta-analysis. J Dent. 2024;142:104843. doi:10.1016/j.jdent.2024.104843 Systematic Review
- Kang SH, Kim BS, Kim Y. Cracked teeth: distribution, characteristics, and survival after root canal treatment. J Endod. 2016;42(4):557-562. doi:10.1016/j.joen.2016.01.014 Prospective Study
- Leong DJX, de Souza NN, Sultana R, Yap AU. Outcomes of endodontically treated cracked teeth: a systematic review and meta-analysis. Clin Oral Investig. 2020;24(1):465-473. doi:10.1007/s00784-019-03139-w Systematic Review
- Berman LH, Kuttler S. Fracture necrosis: diagnosis, prognosis assessment, and treatment recommendations. J Endod. 2010;36(3):442-446. doi:10.1016/j.joen.2009.12.018
- Lubisich EB, Hilton TJ, Ferracane J. Cracked teeth: a review of the literature. J Esthet Restor Dent. 2010;22(3):158-167. doi:10.1111/j.1708-8240.2010.00330.x