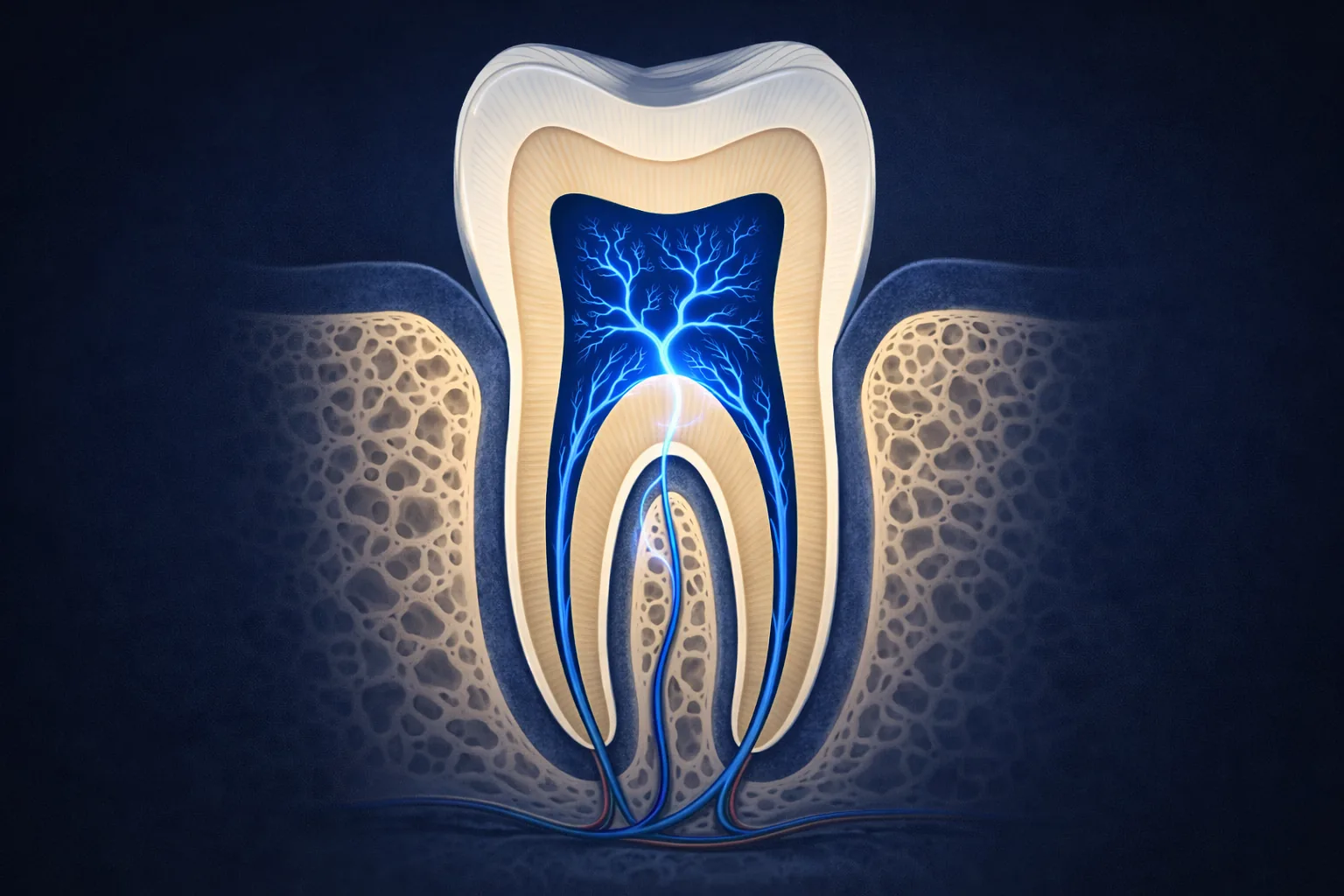
Tooth decay reaches the nerve by dissolving through the tooth's layers: first the outer enamel, then the softer dentin (inner tooth layer), and finally into the pulp (the nerve- and blood vessel-containing chamber inside the tooth). Once decay enters the pulp, root canal therapy is needed — a filling is no longer sufficient to treat the infection.
Tooth decay reaches the nerve by progressively dissolving its way through the tooth’s layers, first through the outer enamel, then through the dentin, and finally into the pulp (the soft living tissue inside the tooth, containing nerves and blood vessels) chamber (the hollow space inside the crown of the tooth that houses the nerve and blood vessels) where the nerve tissue lives. This process is driven by acid-producing bacteria and can take months to years depending on cavity size, bacterial activity, diet, and individual tooth anatomy. Once decay enters the pulp, a filling is no longer sufficient, root canal treatment is needed to remove the infected tissue and save the tooth.
Most people know that cavities can eventually cause severe tooth pain, but fewer understand exactly how that journey happens inside the tooth. Understanding the progression from a small cavity to a painful infection helps explain why catching decay early matters so much. What is happening when a dentist says the decay has “reached the nerve.” Understand why treating decay early prevents far more complex procedures. More on what the root canal procedure involves once decay reaches the pulp.
The Four Stages of Decay Progression
Initial Demineralization and Enamel Decay
Stage 1. Enamel Decay begins when acid-producing bacteria, primarily Streptococcus mutans, metabolize dietary sugars and produce acids that dissolve the mineral content of enamel. Early-stage enamel decay appears as a white chalky spot (white spot lesion) before a visible cavity forms. At this stage, the process can often be reversed with fluoride and improved oral hygiene. The tooth feels nothing, enamel has no nerve supply.
Treatment: Fluoride / remineralization, no filling needed if caught here
Decay Enters the Dentin Layer
Stage 2. Dentin Once decay breaks through the enamel surface, it enters the dentin, the softer, more porous layer beneath. Dentin tends to break down faster than enamel because it is less mineralized and contains the microscopic tubules that lead toward the pulp.2 At this stage, the tooth often becomes sensitive to cold, sweet, or pressure as stimuli travel through the exposed tubules toward the nerve.3 Crucially, dentin decay can spread laterally as well as vertically, a small entry point can conceal a much larger cavity beneath the enamel surface. See signs that decay has reached the nerve and treatment is needed.
Treatment: Filling, pulp can still be preserved if caught here
Deep Dentin Decay. Pulp at Risk
Stage 3. Approaching the Pulp As decay approaches the pulp, the thin remaining dentin offers less buffering between the bacterial front and the pulp’s nerve tissue. The pulp begins to mount an inflammatory response, sometimes producing reparative dentin in an attempt to wall off the advancing bacteria. Pain becomes more pronounced and may start occurring spontaneously. At this stage, the clinical question becomes whether the pulp can survive the insult or has crossed into irreversible inflammation. A deep filling or pulp cap may be attempted in carefully selected cases, but close monitoring is essential.

Treatment: Deep filling or pulp capping, root canal may still be avoidable in select cases
Decay Reaches the Nerve
Stage 4. Pulp Involved When decay breaks through into the pulp chamber, bacteria have direct access to the living nerve and blood vessel tissue. The pulp becomes infected, inflamed, and progressively dies. This produces the characteristic spontaneous, throbbing pain of irreversible pulpitis (severe inflammation of the tooth’s inner tissue, too damaged to heal on its own), or in some cases, a surprising silence as the pulp dies completely. Either way, the infection does not stop at the pulp, it spreads through the root canals toward the root tip, where it enters the surrounding bone and forms a periapical (relating to the area surrounding the very tip of a tooth’s root) abscess (a pocket of infection at the root tip of a tooth, caused by bacteria spreading from inside the tooth).4 Root canal treatment is now required to eliminate the infection and save the tooth structure.
Treatment: Root canal treatment, a filling is no longer sufficient
Why Decay Progresses Without Pain Until It’s Deep
One of the most clinically significant facts about tooth decay is how little warning it provides in its early stages. Enamel has no nerve supply. Stage 1 and early Stage 2 decay produce no symptoms whatsoever. Patients can have a significant cavity developing for months with zero awareness. By the time pain appears, decay has almost always already entered the dentin. By the time pain is severe and spontaneous, decay has usually reached the pulp.
This is precisely why regular dental X-rays, which can detect interproximal (between-teeth) decay long before symptoms or visible signs appear, are the primary tool for catching cavities at the fillable stage rather than the root canal stage.

How Fast Does Decay Progress to the Nerve?
The timeline varies widely between individuals and teeth, and the speed often picks up once decay crosses from enamel into dentin. Factors that can accelerate progression include:
- High sugar and acid intake, frequent feeding of decay-causing bacteria
- Dry mouth (xerostomia), saliva normally buffers acid and remineralizes early decay
- Poor oral hygiene, allows bacterial biofilm (a structured community of bacteria that sticks to tooth and canal walls and is more resistant to disinfection than free-floating bacteria) to accumulate and persist
- Large existing restorations, weaken tooth structure and may allow secondary decay beneath margins
- Teeth with deep grooves or pits, harder to clean and more susceptible to bacterial colonization
- More active bacterial strains, some individuals harbor more aggressive decay-causing bacteria
In a higher-risk individual with a high-sugar diet and poor hygiene, decay can move from enamel into the deeper tooth over a relatively short span. In a lower-risk individual, the same cavity might develop slowly over a longer period and be caught and filled long before causing symptoms. Long-term radiographic follow-up shows this two-speed pattern clearly: the early enamel stage tends to be slow, while the step from outer dentin into deeper dentin moves notably faster, which is why early detection and timely fillings matter so much.1
The Painless Cavity That Becomes an Emergency
The most common scenario leading to an emergency root canal is a cavity that was painless for a long time, was either missed or postponed. Then progressed to the pulp, producing sudden, severe pain that brings the patient in urgently. This sequence is largely preventable with routine dental care and timely treatment of identified cavities. A filling placed at Stage 2 costs less than a root canal, takes less time, and avoids the associated discomfort entirely.
The progression of carious lesions through tooth structure is well characterized in the dental literature. In a long-term radiographic study of young adults followed over a six-year period, lesions that had reached the dentin progressed toward the deeper dentin far faster than early lesions advanced through the enamel: the median time for an outer-dentin lesion to reach deeper dentin was roughly a year and a half, compared with several years for an early enamel lesion to first reach the dentin.1 This faster movement through dentin is consistent with its lower mineral density and the presence of dentinal tubules (microscopic fluid-filled channels in the dentin that transmit temperature, pressure, and sweet stimuli to the nerve) that facilitate bacterial penetration,2 and it underscores the clinical importance of intercepting decay at the enamel stage through routine radiographic monitoring and prompt restorative intervention.
If you have a cavity that has been growing for a while, early treatment is still the simpler path. An endodontist at your nearest MFE location can assess how far it has progressed. Find a location.
Works Cited
- Phillips M, Bernabé E, Mustakis A. Radiographic assessment of proximal surface carious lesion progression in Chilean young adults. Community Dent Oral Epidemiol. 2020;48(5):409-414. doi:10.1111/cdoe.12552 Prospective Study
- Mjör IA. Dentin permeability: the basis for understanding pulp reactions and adhesive technology. Braz Dent J. 2009;20(1):3-16. doi:10.1590/s0103-64402009000100001
- Brännström M. Sensitivity of dentine. Oral Surg Oral Med Oral Pathol. 1966;21(4):517-526. doi:10.1016/0030-4220(66)90411-7
- Ricucci D, Siqueira JF. Biofilms and apical periodontitis: study of prevalence and association with clinical and histopathologic findings. J Endod. 2010;36(8):1277-1288. doi:10.1016/j.joen.2010.04.007